Demyelination
At birth, relatively few pathways have myelin insulation. That is why a baby’s movements are uncoordinated. Myelination in the human brain continues from before birth until at least 20 years of age. Up until the age of 10 or so, vast areas of the cortex are not yet myelinated, and up to the age of 20, large areas of the frontal lobes are not yet myelinated.
The brain’s highly active cells, with high rates of oxygen consumption, produce many free radicals or reactive oxygen species (ROS). Normally, these free radicals are neutralized by antioxidant small molecules (that is, vitamins C and E, urate, glutathione, selenium etc.), as well as protein defense molecules (e.g., superoxide dismutases, catalases, peroxidases, metallothioneins, etc.). Today, especially in stressed-out children and their parents, a wide variety of insults (e.g., sleeplessness, worry, anxiety, hypoglycemia, dysbiosis, hyperactivity, EMF exposure, cell phones, heavy metal toxicity, trauma, seizures, etc.) set in motion a cascade of events that can lead to an excess of free radicals that overwhelm defense mechanisms resulting in tissue and DNA damage unless significant antioxidant supplements are supplied. Without a doubt, the best choice is M-----------’s A----------O and additional selenium. The brain is extremely vulnerable to free-radical-induced damage because it has high oxygen consumption, relatively low defense capability, and large amounts of unsaturated lipids.
Myelin is highly enriched in iron (LeVine, 1991; Erb, Osterbur and LeVine, 1996), which can catalyze the formation of hydroxyl radicals, cause secondary initiation of lipid peroxidation, and/or react with some proteins and EMF radiation, particularly cell-phone usage, to promote oxidative damage, including DNA single and double strand breaks. In lesion sites of multiple sclerosis brains, iron has been found in macrophages and microglia (LeVine, in press). Products of free-radical damage also have been identified in lesion sites (LeVine and Wetzel, in preparation). In one study, high antioxidant intake stopped the damage, including that to the DNA!
The history of studies on vaccines began in 1922 when a smallpox vaccination program caused an outbreak of encephalitis, with a secondary result of Guillain-Barre Syndrome, an ascending paralysis ending in death. The poliovirus produces a breakdown of the myelin sheath, called poliomyelitis, which results in paralysis. Encephalitis, whether caused through disease or because of vaccination, can cause demyelination of the nerves. In regions in which there is no organized vaccination of the population, general paralysis is rare. It is impossible to deny a connection between vaccination and the encephalitis that follows it.
In 1935, Thomas Rivers discovered “experimental allergic encephalomyelitis (EAE)”. Until then, it was assumed that encephalitis was caused by a viral or bacterial infection of the nervous system. Rivers was able to produce brain inflammation in laboratory monkeys by injecting them repeatedly with extracts of sterile normal rabbit brain and spinal cord material, which made it apparent that encephalitis was an allergic reaction. EAE can explain the association of allergies and autoimmune states with encephalitis.
In 1947, Isaac Karlin suggested that stuttering was caused by “delay in the myelination of the cortical areas in the brain concerned with speech.” In 1988, research by Dietrich and others using MRI imaging of the brains of infants and children from four days old to 36 months of age found that those who were developmentally delayed had immature patterns of myelination.
In 1953, it was realized that some children’s diseases,
measles in particular, showed an increased propensity to attack the central
nervous system. This indicated a growing allergic reaction in the population
to both the diseases and the vaccinations for the diseases. There is a
“cure” for measles. It is called vitamin A, specifically, cod-liver oil. As
early as 1932, doctors used cod-liver oil to reduce hospital mortality by
58%, but then antibiotics became the treatment of fashion (Clin. Infect.
Dis., Sept. 1994, pg. 493), and vitamin A was ignored until 1980. A 1993
study showed that 72% of hospitalized measles cases in
In 1978, British researcher, Roger Bannister, observed that the demyelinating diseases were getting more serious “because of some abnormal process of sensitization of the nervous system.” Some investigators believe that vaccination programs are enhancing this increased sensitization of the population.
Dr. Vijendra Singh (now at the
Dr. Singh stated, “We found evidence of brain, serotonin-receptor antibodies in Obsessive Compulsory Disorder patients who were not on any therapy. Those who were on serotonin re-uptake inhibitor therapy did not have these autoantibodies. In other words, the therapy was actually altering the autoimmune response which resulted in improved symptoms.”
Among 33 autistic children (less than or equal to 10 years of age) compared to 18 age-matched, normal children, antibodies to myelin basic protein were found in 19 of 33 (58%) sera (blood serum samples) from autistic children as compared to only 7 of 50 sera from control children. Myelin sheath (the fatty acid complex that surrounds the axons of nerves) is derived from the amino acid serine (with the help of vitamin B12). A serine deficiency is seen in candidiasis and hypoglycemia. Defects in serine synthetic pathway can lead to neuropathy, neuritis, or behavioral disorders, and can mimic folate or vitamin B12 neurological deficiency symptoms.
Dr. Singh stated in part: “Let me touch on the various autoimmune treatments being used for autism. I think they have implications for other neuropsychiatric disorders such as COD (sic - OCD?), and perhaps Torero’s (Long Distance Runner’s) Syndrome. At least two seem particularly promising. One is IVIG—intravenous, immunoglobulin therapy. IVIG is used in immune disorders to replace antibodies that are low in number, as in bone marrow transplant patients where everything is wiped out, or it is used to modulate the immune system. It is expensive and requires treatment on a regular basis, perhaps every 6 or 8 months. IVIG was originally designed for patients with viral infections and severe combined immune deficiencies. The purpose of this treatment is to reconstitute the immune response. It is generally done by bringing immunoglobulin levels to normal status.
“IVIG can be administered at a hospital or a medical center. Even though it is a very safe procedure, there is always a rare chance of adverse reactions especially after long-term use. This was noted in a couple of patients with the neurological disorder Guillain-Barre Syndrome, and there was one case report where after ten years of treatment the patient in his late 40s had an acute reaction. Aside from that, it is a reasonably safe treatment.
“For autistic children, IVIG was first used by Dr.
Sudhir Gupta at the
“You will not find the therapy available everywhere. Remember, it is an experimental treatment. Not every physician who deals with autistic children is familiar with this research. Physicians dealing with autism may not get involved in the autoimmune function with autism unless they have been to a conference on the topic or decided to review the literature.”—Dr. Vijendra Singh. Ph.D.
Actually, the results are not all that exciting for nine out of ten (at a cost for four infusions of about $8000.00, and prospects of having to use it indefinitely to maintain any gains) as this abstract shows: Intravenous immunoglobulin treatment of children with autism. J Child Neurol 1998 Feb; 13 (2): 79 – 82.
“Ten autistic children with immunologic abnormalities, demonstrated on blood tests, were enrolled in this study. Intravenous immunoglobulin, 200 to 400 mg/kg was administered every 6 weeks for an intended treatment program of four infusions. In five children, there was no detectable change in behavior during the treatment program. In four children, there was a mild improvement noted in attention span and hyperactivity.…in one child there was a very significant improvement, with almost total amelioration of autistic symptoms over the time period of the four infusions.”
IVIG, or intravenous immune globulin, is a mixture of immunoglobulins (antibodies), and is prepared from pooled, human-blood plasma. Donors are screened for potential viral infections like AIDS and Hepatitis A and B, but there is a significant risk of occult (hidden) viral infection, especially Hepatitis C, from IVIG. Additionally, “This IgG therapy can be used with patients with low IgA values, but if the IgA values are so low that they cannot be detected, giving IgG therapy is too risky. It is possible the deficient person’s body would produce antibodies against the IgA in gamma globulin, causing potentially fatal anaphylactic shock.”—Dr. William Shaw. For this reason, either Bovine colostrum or Transfer Factor™ (both rich in IgA) should be used before using the IVIG method of restoring the immunoglobulins.
Dr. Singh continued, “There are two other approaches
that I think are important, but I must emphasize the clinical treatment is
not well established. One is the use of immune-suppresser, anti-inflammatory
agents, namely steroids such as ACTH or prednisone. This is a conventional
approach to treating autoimmunity. I have heard from a number of parents of
autistic children that their child was given steroids soon after the
diagnosis, and symptoms improved. The treatment was later discontinued
because they were concerned there could be toxicity on a long-term basis,
and I understand that. But if an autoimmune factor for autism is determined
through research, then there may be some room for treating children with
steroids. There was one study from
“The other treatment is based on anecdotal reports: Sphingolin™ is a trade name for a bovine, brain-myelin preparation. This commercial product is sold as a nutritional supplement, and can be used to correct the immune response against the myelin-basic protein. So, if the child is found to have antibodies to myelin-basic protein or neurofilaments, which are rich in myelin components, then you may think about giving this treatment. Many of those who have done so are noticing very positive responses. Dosage should be quite low to have this benefit to the patient. I’m not a physician and don’t prescribe treatment, but from a research standpoint, the adult dose is generally two capsules per day, hence the child would take only one or one-half. I have parents who insist they would not consider taking their autistic child off this treatment. The important thing is to first check whether the child has antibodies to myelin-basic protein or neurofilament. If there are no antibodies, don’t do this treatment.”—Dr. Vijendra Singh. Ph.D. Interestingly, one study using red-blood cells found that a deficiency of magnesium appeared to alter the fluidity of the cell membrane changing its permeability and making it more susceptible to destruction. This was caused by a significant reduction of a vital membrane lipid (sphingomyelin) apparently resulting from the magnesium deficiency; just one more reason to supplement this vital mineral.
Dr. Hugh Fudenberg had this to say, “With IVIG, only about 15% were helped. These turned out to be the same types in whom we found autoantibodies to myelin-basic protein and other Central Nervous System tissue constituents.” Dr. Jane El-Dahr says, “My concern was always that unless we got to the bottom of why these children had the brain auto-antibodies to begin with, high-dose IVIG would be only temporarily effective and not a long-term solution. Once I began reading about mercury and autoimmunity, especially about brain autoantibodies in workers exposed to mercury, things started to make sense.”
To all this I ask, “Shouldn’t we use S---------™, or better, a combination of Colostrum, A------------™, and L--------™ first?” Though slower acting, they accomplish the same basic purposes as IVIG without the risk or the prohibitive costs and the results can be sustained.
In 1993, Vijendra Singh, PhD, published a study in which they found antibodies to myelin-basic protein in 50 to 60% of autistic children tested. In 1988, research by Dietrich and others using MRI imaging of the brains of infants and children from four days old to 36 months of age found that those who were developmentally delayed had immature patterns of myelination. Sphingolin™ (Myelin-sheath, protein supplement that is the exact component of the sheath), is available from Terrace International (909-307-2100), $10.95 (1-month’s supply), or from L & H VITAMINS at (800) 221-1152. The Web page for stories of people with MS that have used Sphingolin™ is www.2cowherd.net .
In 2001, Dr. Singh published an abstract stating in part, “Considering MBP autoantibodies as an index of autoimmunity to myelin, an open-label trial of oral Sphingolin™ is under assessment—preliminary results are encouraging with significant improvement of behavioral characteristics in the autistic people.”
Since antibodies persist for a much longer period of
time than antigens of nucleic acids, the detection of antibodies may be a
reflection of past infection no longer active. Caution needs to be applied
in the interpretation of antibody studies. The need for caution derives from
the fact that some infectious and autoimmune diseases can result in
polyclonal B-cell activation with subsequent secretion of antibodies
directed at a range of infectious and host-derived antigens. For example,
infection with Epstein-Barr virus can result in the development of
antibodies to a number of other viruses including measles, rubella,
adenoviruses, enteroviruses and varicella-zoster virus. Similarly, infection
with human immunodeficiency virus results in the development or augmentation
of antibodies to a range of viral antigens as well as to host-derived
antigens such as DNA, myosin, and ovalbumin. It is thus possible that the
detection of antibodies to a range of viral agents may reflect infection
with a more limited repertoire of infectious agents. Similarly, the presence
of antibodies to host-derived proteins, noted in previous studies of
schizophrenia, may reflect infected cells, as well as autoimmune pathogenic
mechanisms. (Pathogenetic Aspects of Infectious, Immunological, and
Chronobiological Processes in Psychiatric Diseases,
Henneberg AE, Kaschka WP (eds): Immunological Alterations in
Psychiatric Diseases. Adv Biol Psychiatry,
This recent study adds significant new input into the myelin discussion:
A new view of multiple sclerosis (MS) may arise from
the first extensive study of brain tissue from the earliest hours during a
bout of the disease. The results, published February 23, 2004, in the
advance on-line edition of the Annals of Neurology, suggest that the
earliest event is not, as previously believed, a misguided, immune-system
attack on a brain substance called myelin. Instead, the first event appears
to be the death of the brain cells that produce myelin, triggering a
subsequent immune system mop-up operation to clean up the cells and the
myelin, said author John W. Prineas, MBBS, of the
“This patient proved to be unique in the history of multiple sclerosis in that there was lesion available for study that was less than a day old,” said Prineas. Prineas and Barnett noticed that the myelin in the lesion was still intact, and there was no evidence that the typical armada of immune system cells and molecules had moved into the area yet. Instead, oligodendrocyte cells, which produce the myelin, were dying. Myelin is, in fact, an extension of oligodendrocytes that wrap themselves around nearby nerve fibers.
“This encouraged us to re-examine other early MS cases in our brain bank,” said Prineas. “Similar lesions, albeit extremely rare, were identified in a number of other early MS cases, which allowed us to conclude that the changes observed probably occur at the onset of any typical new lesion.” The results could have significant consequences for MS research, much of which is focused on understanding why the immune system attacks myelin. The focus needs to shift to understanding why the myelin-producing cells begin to die.
As to steroids, a personal view is that at no time, except to save a life is steroids justified for a child. If continued, as would be necessary for any long-term benefit, the side effects will be worse than the condition treated. Furthermore, with IVIG, a human blood product goes directly into the veins. It must be prepared and processed differently than IMIG (Intramuscular). Some people will get a little better from IVIG, because a dysfunctional immune system is the culprit for these children’s problems, and this product can help the immune system. The trouble is that it is not a sustained gain. There is a very real danger of passing hepatitis and/or any number of unidentified retroviruses with this type of therapy. Presently we have no reliable screens for hepatitis C, D, E, F, or G. If there is an allergic reaction in a child with low IgA, the possibility of either getting very sick, or even dying is very real. Mentioned in this paper are a number of safer ways to restore the immune function. These should be used before resorting to the very expensive, potentially dangerous, IVIG.
 This
interesting snip from a recent study that determined that a tiny amount of a
“sugar” attached to the IgG molecule accounts for the beneficial results of
IVIG:
This
interesting snip from a recent study that determined that a tiny amount of a
“sugar” attached to the IgG molecule accounts for the beneficial results of
IVIG:
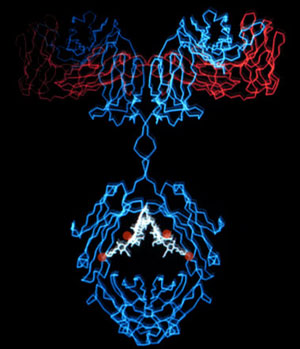
A small fraction of the IgG antibodies in the IVIG solution carry a sugar called sialic acid that is required for its protective ability. This accounts for the large amounts of’IVIG needed.
“This is a very interesting condition that’s set up,” Jeffery Ravetch, Leonard Wagner Laboratory, says. “IgG can shift from a state that is quite inflammatory to a state that is actively anti-inflammatory by just changing this sugar.” This switch occurs during a normal immune response to a foreign substance, shifting the IgG antibodies from an anti-inflammatory state to one that is pro-inflammatory and able to efficiently dispose of the foreign challenge.
They found that just enriching IgG species with this sugar increased IVIG activity by a factor of ten, while removing it wiped out the therapeutic activity altogether! It is interesting to note that a molecule of galactose (mostly found in milk) missing from the end of these IgG molecules will cause arthritis. (A---------- A-----------e® contains significant amounts of both these sugars.)
The four red dots are the sialic (neuramenic) acid within the IgG molecule in its anti-inflammatory mode.
It is recognized that many of the ASD children do
indeed have myelination problems probably from vaccine damage. Strong
evidence that these vaccines cause myelin sheath damage (multiple sclerosis)
has caused
One variation of serine, namely Phosphatidylserine, serves several important functions within the central nervous system, including development of the myelin sheath. Phosphoserine, a modification of serine, is a good predictor of vitamin B6 deficiency, in particular the form of vitamin B6 called Pryidoxal-5-Phosphate (P5P). If plasma Phosphoserine levels are abnormally high, that is a clear indication of P5P deficiency. P5P is critical in amino acid processes. Tyrosine, for example, cannot be converted into the neurotransmitter norepinephrine if there is not enough P5P. Likewise, tryptophan cannot be converted into the neurotransmitter serotonin if there is not enough P5P. An excess of serine and threonine, however, is seen in vitamin B6 deficiency. Vitamin B6 often is not being converted to P5P because of a lack of magnesium!
This MBP damage can be ameliorated, further damage prevented or repaired through nutritional intervention and the removal of heavy metals. Specifically, by supplementing lecithin, and using the other nutritional interventions mentioned herein. Lecithin, though from soy, does not have the negative qualities of soy for it does not contain those negative substances of soy protein, copper, diadzen, and genistein. Lecithin has proved useful in the following conditions:
- It prevents cholesterol from congealing in fatty clumps in the blood and attaching to the vessel walls. It lowers the “melt” point from something like 180 degrees Fahrenheit to somewhere in the range of 65-75 degrees, fully liquid in the blood.
- Exhibits good antioxidant properties.
- Supplies choline that is so necessary to proper use of fats, and which increases available acetylcholine in the brain. A lack of acetylcholine produces urinary retention, gastric reflux, reduced cognitive function, and myasthenia gravis. Manganese, methionine, and inositol work with choline to produce lecithin in the body.
- Detoxifies lead, mercury, various drugs, and counteracts the effects of radiation and DDT, and neutralizes many poisons. It protects and repairs myelin sheath of nerve fibers damaged by heavy metals and toxins—neutralizing or minimizing the effects of nitrates and nitrites.
- In cancer treatment, it prevents melena (blood in the stool from radiation damage).
- Dr. Minea achieved improvement in 80% of MS patients with injections of lecithin. Copper is also needed for myelin sheath.
- With the B-vitamins, rutin, calcium, magnesium, and unsaturated fatty acids, it gives relief of shingles.
- With vitamin E, it reduced insulin requirements of diabetics in several patients.
- Aids in protecting the eyes.
- Lecithin and antioxidants should accompany supplemental fatty acids.
-
Being high in phosphorus, it can imbalance calcium if coupled with an
intake of soft drinks, meats, and phosphate additives in processed
foods. Studies in
Suggested: up to four tablespoons of granules in cancer and MS. Good food sources: eggs, seeds, and cold-pressed oils. See www.centralsoya.com/CENSOYA/LECITHIN.NSF for additional information on lecithin.
While it is not my purpose to study diets in detail, I
would like to observe that one should not concentrate on one food such as
soy, rice, or nut milk, but use as great a variety as is available, for all
of these have definite deficiencies as the perfect food. Soy infant formula,
for example, raises blood levels of estrogen thousands of times higher than
breast milk (Alternatives Vol. 8, No.3, Dr. David G. Williams), and contains
enzyme inhibitors that can affect the thyroid adversely. It is also high in
copper that slows the thyroid. Dr. Jonathan Wright’s “Nutrition and
Healing”, April 2001 states; “One ounce of soy a day for one month can
result in a significant increase in ‘TSH’ (the hormone that increases with
hypothyroidism). The FDA subsequently found that diadzen and genistein (two
of the most ‘hyped’ soy isoflavones) are responsible for this hazard.” In
fact, scientists Daniel Sheehan and Daniel Doerge, from the
The frequency of feedings with soy-based milk formulas
in early life was significantly higher in children with autoimmune thyroid
disease (prevalence 31%) as compared with their siblings (prevalence 12%).
It can also decrease the ability of red blood cells to absorb oxygen
according to Dr. David Williams and Dr. John R. Lee in their newsletters.
There’s concern about the fluoride level, the estrogen level, the manganese
level, and the glutamate level in these soy infant formulas. Its
phytoestrogens require sulfate to solubilize them to remove them from the
body; thus, a PST child should avoid soy products that are unfermented. Soy
is also highly allergenic. Soy infant formula is high in both fluoride and
aluminum, far surpassing the “optimal” dose, and has been shown to be a
significant risk factor in dental fluorosis. If the formula is combined with
fluoridated local water, the problem is compounded. Aluminum greatly
potentiates fluoride’s effects on G-protein activation, the on/off switches
involved in cell communication and of absolute necessity in thyroid hormone
function and regulation. Both organic and inorganic fluoride compounds have
been shown to inhibit zinc-containing enzymes, such as carbonic anhydrase
(Dugad et al., 1988,1989; Gelb et al., 1985) that is also now used as a
marker for thyroid dysfunction (Hori et al., 1998). Additionally, fluoride
bonds with magnesium in the blood into the insoluble magnesium fluoride.
This means that the magnesium cannot be assimilated by the pituitary, with
the consequent failure of the pituitary to function properly that leads to
the symptoms of magnesium deficiency.
Soy is lacking also in the essential, sulfur-bearing, amino acid, methionine. Methionine is a critical nutrient for infants and children for growth and tissue development. They require 22 mg/kg per day for proper growth and development. Adults need only half that! D-L-methionine is an anti-inflammatory and an antioxidant, and it metabolizes into several other sulfur, amino acids (Cysteine, Glutathione, and Taurine) that support the body’s natural detoxification pathways. Adequate methionine, if metabolized into these amino acids, ensures detoxification of mercury, arsenic, and lead. It is an anti-inflammatory aid to arthritis, fibromyalgia, headaches, migraines, and other chronic pain syndromes. Both Asian and Western children who do not get enough meat and fish products to counteract the effects of a high phytate diet, frequently suffer rickets, stunting, and other growth problems due to a lack of methionine and an induced zinc deficiency.
This induced deficiency of zinc will cause children to absorb more aluminum into their systems, because aluminum competes with zinc in binding sites on ligands, organic molecules in the body that attach to a single metallic ion. Systemic reduction of zinc is especially prevalent in infants fed with soy formulas. [Settle et al., “Effect of phytate: zinc molar ratio and isolated soy bean protein on zinc bioavailability”, Journal of Nutrition, Vol 111, 1981, p.2223-2235.] Methionine is a critical nutrient for infants and children for growth and tissue development. They require 22 mg/kg per day for proper growth and development. Adults need only half that! D-L-methionine is an anti-inflammatory and an antioxidant, and it metabolizes into several other sulfur, amino acids (Cysteine, Glutathione, and Taurine) that support the body’s natural detoxification pathways. Adequate methionine, if metabolized into these amino acids, ensures detoxification of mercury, arsenic, and lead. It is an anti-inflammatory aid to arthritis, fibromyalgia, headaches, migraines, and other chronic pain syndromes. Both Asian and Western children who do not get enough meat and fish products to counteract the effects of a high phytate diet, frequently suffer rickets, stunting, and other growth problems due to a lack of methionine and an induced zinc deficiency.
Rice, in many of its forms, is a high-glycemic food that elevates insulin in an undesirable fashion, and when coupled with the plethora of other high-glycemic foods found in the American diet, is very detrimental to blood sugar control and fatty acid metabolism. Furthermore, different brands of rice milk vary widely in sugar/carbohydrate content. Shop carefully, and rotate these foods to minimize blood sugar problems and allergic potential. “While I agree with the anti-milk stance, it is important to remember that people should NOT switch to soy milk or rice milk”—Dr. Joseph Mercola. His reasons, in addition to those listed above, is that some soy milk products do not have sufficient vitamin D for toddlers, and some rice-based milks do not have enough protein. Look into Hemp milk.
When one ingests sugar or high glycemic foods, insulin is released from the pancreas to assist the sugar into cells and to control blood sugar levels. Balancing this action, the adrenal glands release catecholamine hormones (epinephrine and norepinephrine) to keep the sugar levels from dropping too low. Studies have revealed that ADHD children (and autistic who are ADHD) release only half as much of the catecholamines as normal children. Norepinephrine plays a vital role in attention and ability to focus. We also know that dopamine plays a vital role in performance and memory. Serotonin deficiency appears to play a vital role in violent and antisocial behavior. This drop in neurotransmitter activity will allow a drop in blood sugar that creates a significant decrease in brain activity in these children. Sugar is poison to these children, and a removal of sugar and high glycemic foods will make a great difference in their behavior. Avoiding these poisonous foods, and strengthening the adrenals will often correct the problem. One aid in supporting the adrenals that is recommended by Dr. David Williams is Drenamin™ by Standard Process Products™ (800-848-5061). Other adrenal glandular products are available at your health food store, and the nutrients needed are listed herein.
Acetyl L-carnitine (ALC) is the acetyl ester of carnitine (an amino acid) that transports fats into the mitochondria. In the mitochondria these fats are converted to energy. ALC not only increases the synthesis and release of acetylcholine, it now appears that it has neuroprotective and neuroenhancing properties as well. We’ve noted that the enzyme CoA is needed to convert choline to acetylcholine. S-Adenosylmethionine (SAM) is also an enzyme that is important in acetylcholine synthesis. Stimulation of the parasympathetic nervous system releases acetylcholine at the nerve endings. Loss of gut mucosal integrity (common in ASD) would decrease by 85% gut absorption of CoA, shunting choline into homocysteine production that folic acid, vitamin B6, and B12 metabolize back into usable aminos. TMG helps make SAM.
Dimethylaminoethanol (DMAE) is a safe, natural substance that easily crosses the barriers in the brain and nerve cells where it is converted first to choline and then to acetylcholine. It is an MAOI, and requires special consideration when using dopamine enhancement. DMAE, often referred to as a Smart Nutrient, is a very efficient antioxidant and free-radical deactivator. It stabilizes lysosome membranes preventing leakage of collected toxins and protein-damaging enzymes. Increased production of acetylcholine may explain why a continuous dietary source of SAM or DMAE makes people with multiple disorders feel better. Many will profit from this increase of acetylcholine, but observe the earlier mention of where too much, or an imbalance with norepinephrine, can cause adverse effects. Kane has observed bad effects of multiple vitamins containing choline. The affected group would likely be those unable to absorb CoA, and those suffering allergies, yeast overgrowth, and PST/sulfoxidation disorders.
Not to be confused with carnitine or acetyl-L-carnitine is the dipeptide, Carnosine, sometimes presented as N-Acetylcarnosine. Doctor Chez finds most beneficial a dosage of 400 mg Carnosine in combination with 50 IU vitamin E and 5 mg zinc, twice a day. “It affected language, receptive language, eye contact, communication, which are things children with autism have big gaps with (sic),” Chez said. It is interesting to note that, at least for adults, the dose is 1000 mg spread through the day, “for the body automatically metabolizes lower amounts of Carnosine into an inert substance, but the body cannot neutralize the 1000 mg” (Life Extension Directory).
Carnosine is the dipeptide of the amino acids histidine
and alanine, and functions primarily as a pH buffer in muscle tissue.
Unfortunately, muscle levels are reduced 63% between ages 10 and 70
(Stuerenburg). High Carnosine levels are associated with an increase in
physical performance especially anaerobic performance. Carnosine is best
known for its ability to buffer lactic acid in muscle tissue and for its
multiple antioxidant capabilities. When cells were exposed to 90% oxygen,
only Carnosine exerted significant protection. It reduced the level of
chromosomal damage by two-thirds! It boosts levels of free IGF1, a hormone
necessary to maintain youthful cellular function throughout the body. Aging
cells in contact with Carnosine regain a more youthful appearance (McFarland
1999). The present findings would indicate an immunoprotective role of
Carnosine, although definitive conclusions must await the results of future
studies. A study by
In some children, too high a dose of carnosine may overstimulate the frontal lobes which can cause increased irritability, hyperactivity, or insomnia which was observed in hyperactive autistic children. Other than that, there were no side effects, Dr. Chez says. Carnosine can accumulate as a result of high intake with insufficient zinc availability, from excess buildup of beta-alanine (due to unusual bacteria activity in the gut upon aspartic acid, ingestion of high amounts of pantothenic acid (vitamin B5), or due to a lack of vitamin B6. Elevated beta-alanine inhibits the breakdown of anserine and carnosine and impairs the renal conservation of taurine and beta-aminoisobutyric acid. This can be detrimental for taurine is an important antioxidant and a neuroinhibitory neurotransmitter, and it is essential for the retention and homeostasis of intracellular magnesium and potassium. Excess beta-alanine is a neurotoxic substance that suppresses development in the brain and spinal cord, and interferes with metabolism of the other neuroinhibitory neurotransmitter, GABA.
Actually, Dr. Pangborn, Ph. D. biochemist, has some serious reservations about this usage of carnosine:
In body tissues, carnosine is split into histidine and beta-alanine. Beta-alanine can be a real troublemaker, and I’ll get to that shortly. Histidine is the Dr. Jekyll and Mr. Hyde part. Histidine becomes formiminoglutamic acid (FIGlu), and FIGlu (an intermediate metabolite in histidine catabolism in the conversion of histidine to glutamic acid, with the formimino group being transferred to tetrahydrofolic acid) pushes the formation of 5-formiminotetrahydrofolate. A build up of FIGlu usually indicates a folic acid deficiency. (A test of vitamin B12 deficiency, folic acid deficiency, liver disease, or genetic deficiency of glutamate formiminotransferase, based on urinary excretion of FIGlu).
This is good, even though it often raises FIGlu levels in the urine and blood of autistics. It’s good because: (a) it helps remove a potential folate trap, and (b) it leads to two forms of folate that are required for purine and purine nucleotide synthesis. One of these forms, 10-formyltetrahydrofolate, comes in just after the adenylosuccinase step and helps “pull” the process along at a documented sticking point for some forms of autism.
However, histidine and Carnosine are powerful carriers of copper. They transport copper from the intestinal milieu into the portal blood, and from there to organs and tissues in the body. And don’t think you can displace copper with zinc once the copper is on histidine - you cannot. The equilibrium constant for copper II chelated to histidine is 18.3; for zinc it is 6.7 to 12.9, depending on chelate structure (Ref. Chaberek and Martell, Organic Sequestering Agents, John Wiley & Sons, p.549). Because these are exponential relationships, the real difference in the constants is 10 to the 5th up to 10 to the 11th. Only glutathione, cysteine, and thionein can intercept this Carnosine-copper transport, but that’s one of the big problems in autism, isn’t it? These sulfur players have gone AWOL, and copper is excessive at the expense of zinc. Dr. Bill Walsh has made excellent presentations on this. You might think that Carnosine plus zinc will act to put zinc in and take copper out. With these equilibrium constants and with the natural copper content of food, that’s very unlikely. You need a million or more zinc atoms for each copper atom to be competitive in this game! Histidine/Carnosine-copper wisdom has graduated into medical textbooks. We’re not talking about research papers; we’re talking what you should and shouldn’t do per medical texts. Copper homeostasis with histidine and histidine-albumin complexes are well discussed by David Danks, Chapter 58 of Stanbury et al, The Metabolic Basis of Inherited Disease, 5th Ed, p.1252-1254.
For Carnosine, the publicity is a bit worse. Carnosine is a threat to worsened Wilson’s disease because it and its sister anserine are such good importers of copper to body tissues. Ref: Scriver CR and TL Perry, Chapt 26 in Scriver et al eds, The Metabolic Basis of Inherited Disease 6th ed McGraw-Hill (1989) 765.
Now, let’s go to the really bad guy here, beta-alanine. To be concise: beta-alanine blocks renal conservation of taurine and causes hypertaurinuria - loss of taurine in the urine. This, in turn, causes urinary loss of magnesium, which worsens sulfotransferase activity as well as lots of other necessary enzymatic processes. If you give Carnosine, you lose taurine and magnesium. There are lots of references, but you can start with Dr. Charles Scriver’s work referenced above, because all of this biochemistry (Carnosine, beta-alanine, taurine, etc.) is closely related.
Histadine is a powerful chelator and can quickly deplete nutrients already in short supply. Nevertheless, carnosine has been used very successfully in protecting against radiation damage by boosting immune function in cancer patients. So, it is not my purpose to recommend for or against Carnosine usage, but to bring you the pros and cons. I will say that it is touchy enough that it should not be used except under a knowledgable doctor’s supervision.